

The science behind viruses is derived from the germ and contagion theories of disease. Theories updated by Marcus von Plenciz in 1762, but invented earlier by the Venetian Girolamo Fracastoro, in his Latin book written in 1546, De Contagionibus Et Contagiosis Morbis. Gerolamo was educated at Padua University and elected as a physician of the Council of Trent.
His ideas were further expanded upon in 1646 in another Latin work by the Jesuit scholar and polymath Athanasius Kircher. After investigations on Antonie van Leeuwenhoek’s newly invented light microscope, Kircher witnessed “worms” secreting from decaying bodies of meat and milk, leading him to assert that disease and putrefaction (decay) is caused by the presence of invisible living bodies. Upon discovering similar “little worms” or “animalcules” (the name given by Leeuwenhoek to bacteria seen under optical microscopes) in the blood of patients struck during Rome’s 1656 “bubonic plague” period, Kircher apparently concluded that disease was caused by microorganisms. Making him the first person to link infectious diseases to a microscopic pathogen. Outlining his germ theory of disease in Scrutinium Pestis Physico-Medicum, written in Rome in 1658. As it turns out, what he saw under his microscope was in actuality red or white blood cells — not a plague agent. Yet, it was Kircher who proposed many of the hygienic measures adopted today to prevent the spread of the now widely accepted notion of contagious diseases, such as self-isolation, quarantining, burning of clothes worn by the infected, and the wearing of face-masks.
It took up until the last century and the invention of an electron microscope before the existence of viruses could be visually portrayed. Equating to small black blobs of pixels, often mistaken for other biological debris, requiring microscopic specialists to analyse.
Set out in 1890, the gold standard supposed to be used by virologists to determine the microbial cause of infectious diseases has been Koch’s postulates, which state:
- “1) The microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms.
- 2) The microorganism must be isolated from a diseased organism and grown in pure culture.
- 3) The cultured microorganism should cause disease when introduced into a healthy organism.
- 4) The microorganism must be reisolated from the inoculated diseased experimental host and identified as being identical to the original specific causative agent.”
Many will consider this approach as cruel towards animals but essentially Koch’s postulates assert that from a group diagnosed with similar symptoms, the same diseased organism (i.e. the blood or respiratory secretions) should be found, from which a pure culture can be grown and injected into a susceptible animal for infection, so its diseased organism can then be cultured out of them.
Dr Thomas Cowan, author of The Contagion Myth, gives the example of chickenpox: when, typically, children experience low-grade fever, sickness, and a vesicular rash, causing blister bubbles, the fluid from which under a microscope shows thousands to millions of copies of what is referred to as the chickenpox virus. Also contained in abundance within the infected blood, a condition called viremia (similar to bacteremia); in contrast to healthy blood which harbours no such viruses or bacteria. This is a pure culture of chickenpox, not existing to any such extent within the fluid or blood of normal healthy people.
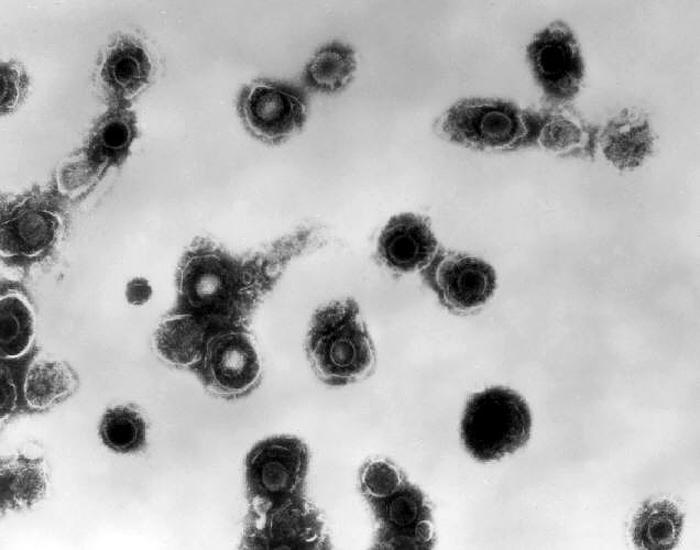
In the case of SARS-CoV-2 (aka COVID-19, or 2019-nCoV), a purported novel mutation of coronavirus (the technical term for common-flu), there is no evidence that Koch’s postulates were fulfilled and that a virus has ever been purified (or isolated). Instead, smears of electron microscopy (EM) examinations were provided from the lung fluid of patients, showing “cellular debris,” a number of which appear like the depiction of viruses, one of which was classified as COVID-19. This is entirely different to demonstrating millions of copies of the virus in the sputum and blood, as is done with chickenpox or meningococcal. And certainly doesn’t fulfil Koch’s postulates.

The claimed source of the viral outbreak was in Wuhan, China, in December 2019, reportedly from a seafood market with unsanitary conditions (although it’s also blamed by some on a nearby lab leak). After examining 198 patients we’re told attended the seafood market, it’s claimed that scientists genetically sequenced coronavirus material as RNA instead of DNA, said by virologists to have been previously unseen, leading them to conclude it must be the cause of this sudden sickness.
Dr Cowan reckons: “This flies in the face of everything we know about virology and infectious causation…and I would also point out this is not the first time this has happened – in fact: it happens every time.”

He goes on to cite a polio outbreak example from the late 1800’s, occurring at the same time orchids and apple trees were sprayed with lead arsenic and later Dithiothreaitol (DTT), both specific poisons now known to affect the anterior horn cells of the nervous system, the pathological area of the body in polio. Causing people to contract symptoms of acute paralysis eventually termed polio.
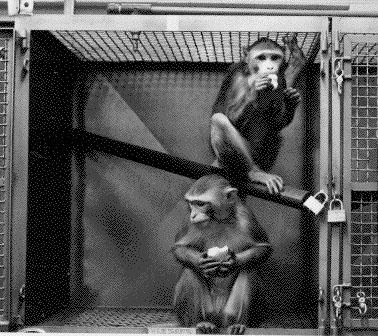
Virologists without access to electron microscopes or any visibility of viruses had to use other methods to try and prove their contagion theories. Dr Cowan describes how they first extracted the diseased spinal chords and brain tissue of dead paralysed children, then blended this material up without any purification, and gave it as a drink to monkeys, but they never got sick. Unable to make any animals sick, they moved onto subcutaneous injection (a shot inserted into the fat layer between the skin and muscle) into the monkeys arms, but still none got sick. Determined to offer some evidence, researchers resorted to drilling holes into two monkeys skulls, then inseminating a quarter cup of spinal chord fluid goop through these skull holes into the brain; one monkey died and the other was paralysed, the latter of which was pictured being held up as proof by a proud researcher.
Dr Cowan notes that this blatant failure of evidence was also the case in relation to the 2009 H1N1 virus (swine flu) epidemic; the H5N1 virus (influenza) detected since 1996; the severe acute respiratory syndrome (SARS) surfacing in the early 2000’s; the hepatitis C virus (HCV) of 1988; the Ebola virus disease (EVD) identified in 1976; and the Zika virus (ZIKV) appearing in 1947.
The procedure which should’ve been carried out for COVID-19, according to Dr Cowan, was to round up a sample of 500 people suffering from its symptoms (a vague low-grade fever and dry cough, also experienced by those with bronchitis, asthma, air pollution, etc., showing up as a shadow on the lungs in a CT scan) for an electron microscopy examination of their sputum and blood, to observe millions of copies of the virus, and characterise it. 100% of this first group should have millions of copies of the virus in their sputum or blood, which can then be weighed against a control group of another 500 healthy people, who shouldn’t. At that point Dr Cowan states that the procedure would be to purify (filter) those millions of copies the virus, and infect it into a susceptible animal (either by injection or squirting it up the nose or down the throat). If all these animals begin showing millions of copies of the virus in their sputum and blood, against a control group given some saline solution that doesn’t develop the virus, then the virus is proven to exist.
The modern tool used for diagnosing coronavirus is called a reverse transcription polymerase chain reaction (RT-PCR), aka, a viral load test. The technique is described by virologists as a combination of reverse transcription of RNA into DNA (in this context referred to as complementary DNA or cDNA) and amplification of specific DNA targets it’s primed with through polymerase chain reaction (PCR). This viral load surrogate test is a theoretical estimation of microbial activity.
PCR was developed by the Nobel Prize winning virologist Kary Mullis to detect HIV. He however recognised limitations and specifically contradicted any usage as a diagnostic test, stating: “Quantitative PCR is an oxymoron. PCR is intended to identify substances qualitatively, but by its very nature is unsuited for estimating numbers. Although there is a common misimpression that the viral-load tests actually count the number of viruses in the blood, these tests cannot detect free, infectious viruses at all; they can only detect proteins that are believed, in some cases wrongly, to be unique to HIV.” “The tests can detect genetic sequences of viruses, but not viruses themselves.”
The PCR tool simply amplifies the biological sequences of purported viral fragments millions of times. It does not demonstrate viremia, or fulfil Koch’s principles by isolating any particular viruses, nor even conclusively identify or detect any virus, according to its own inventor. Who categorically denied it can be relied on to definitively diagnose any viral infection….as it has also been used for in the case of COVID-19. Surrogate data testing is performed by a best assessment of available information and can only be a gold standard test (a diagnostic test benchmark) with necessarily correct assumptions. In the case of chickenpox and meningococcal, for example, Koch’s postulates are considered by the mainstream medical industry to be accurate 100% of the time.
During the PCR process, supposedly “unique genetic sequences” are stimulated to create copies, which multiply with each cycle. After 36 cycles there is a colour change to designate the biological material as positive for coronavirus, although there will still be false positives (an indeterminable amount without comparable data). When it’s carried out 37 times and seen for example 5% of the time within patients suffering related symptoms, then that output is relayed as the final result. However, if 40 – 60 amplification cycles are carried out, lots more sequence samples start testing positive — eventually ending up at 100% at the highest magnification levels.

This would seem to prove that within everybody’s physiological secretions is a piece of the said COVID-19 RNA (as well as the “unique genetic sequences” ascribed to any other viruses). But the PCR tool is reliant on using primers to bind to these sequences, acknowledged to increasingly bind to more non-target sequences and produce more false-positives the higher the amplification levels, due to it increasing background noise (contaminants, dead matter, other biological sequences).

Confusion further arises due to each country using its own standard number of magnification cycles, a figure they may decide to alter during an epidemic, and by that factor alone dramatically increase or reduce the percentage of total infections. Potentially skewing statistical results and enabling intentional manipulation in the promotion or dismissal of specific cures or causes.
Dr Cowan says: “All biological tests have false positives. So, if you test 30 million people and you have a 1% false positive rate, then 300,000 people, by definition, will test positive, and then you have an epidemic.” “And then if you want to demonstrate that the epidemic got better, all you have to do is lower the magnification examples to 35, and then suddenly your vitamin C or vaccine or your chloroquine or whatever you did, worked! And now there’s no more people testing positive.”
These articles form a chapter of The Invisible Enemy book.